
Rib Fracture Missed on Chest X-ray: How Point of Care Ultrasound Changed Management After a Skiing Fall
This case was originally published in the Journal of Urgent Care Medicine. The full article and accompanying discussion can be found here.
Case Overview
A 51-year-old male presented to urgent care after falling while spring skiing. He reported catching an edge, pitching forward, and landing forcefully onto his left anterior chest. He immediately experienced localized pain, worsened by deep inspiration. He denied shortness of breath, syncope, and head or neck injury.
Vital signs were normal. Examination demonstrated focal tenderness over the left anterior chest wall at the level of the fourth rib without visible ecchymosis, crepitus, or deformity. Lung sounds were clear and equal bilaterally.
A chest X-ray showed no acute bony abnormality and no pneumothorax. Due to persistent focal pain, point-of-care ultrasound (POCUS) was performed over the area of maximal tenderness.
POCUS Findings
Using a high-frequency linear transducer, ultrasound evaluation of the left anterior chest wall in the longitudinal plane demonstrated disruption of the normally smooth hyperechoic rib cortex with a subtle step-off deformity. These findings were consistent with a non-displaced fracture of the fourth anterior rib.
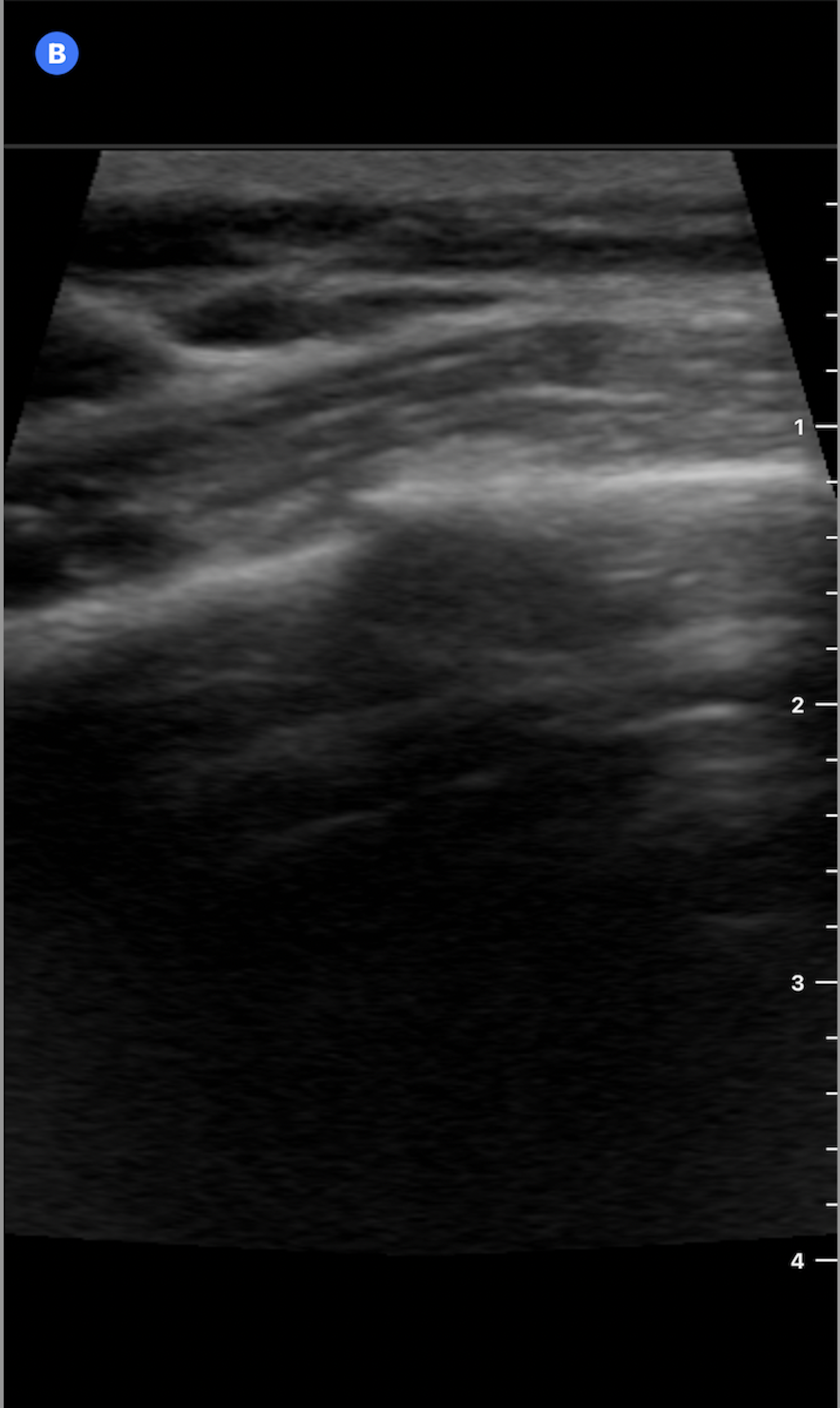
Figure 1: Ultrasound image of the 4th anterior rib in the longitudinal plane without annotation.
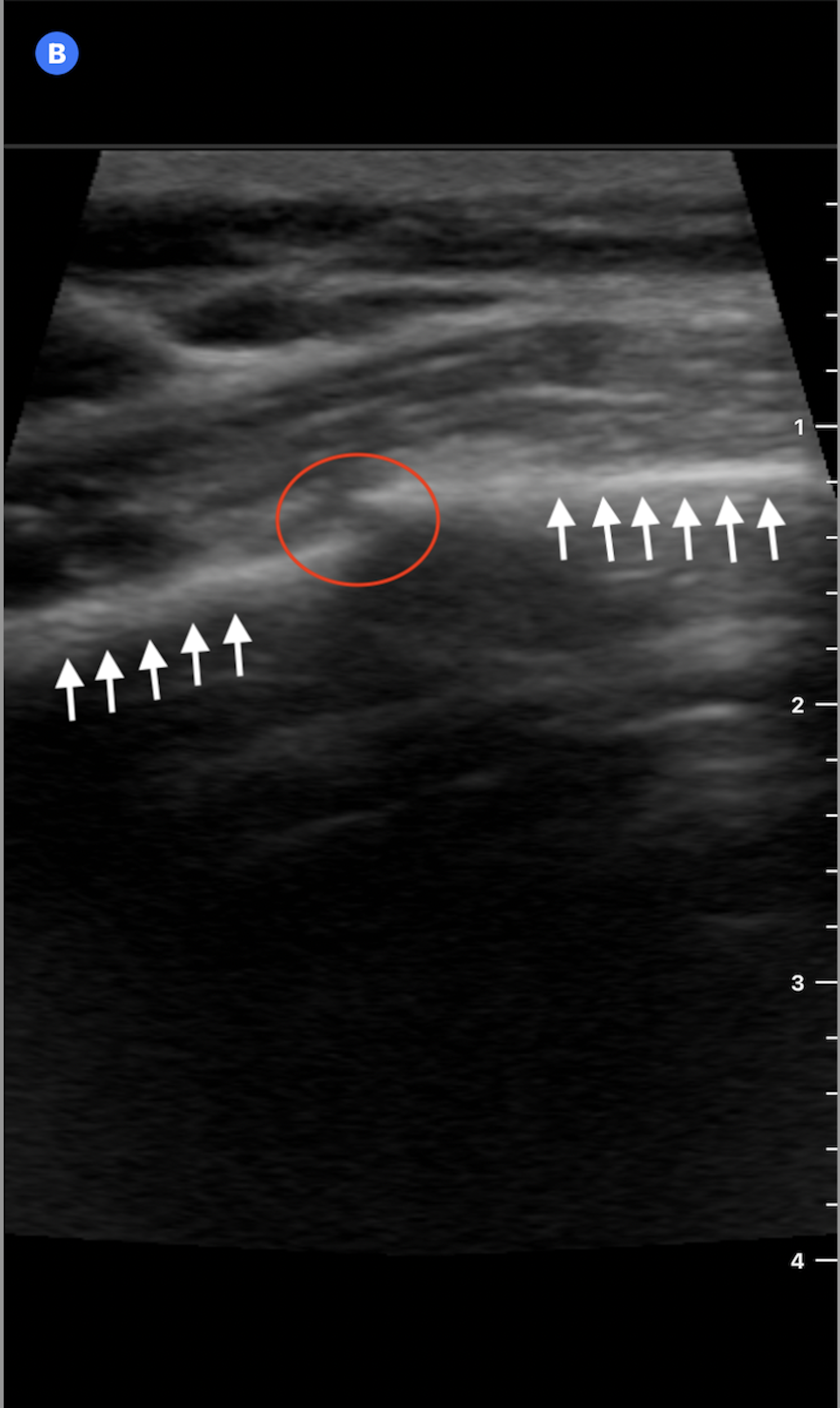
Figure 2: Ultrasound image of the 4th anterior rib in the longitudinal plane shows linear hyperechoic bony cortex (white arrows) with a minimal step-off and discontinuity (red circle) consistent with a nondisplaced rib fracture.
In addition, no surrounding soft tissue hematoma was visualized. Lung sliding was present, and there was no pleural effusion, reducing concern for pneumothorax or hemothorax. Learn more about POCUS for pneumothorax in this article.
Evidence: Ultrasound Versus Chest X-ray for Rib Fracture Detection
Rib fractures are frequently missed on chest radiographs, particularly when fractures are anterior or non-displaced. In a 2022 systematic review and meta-analysis published in Annals of Emergency Medicine, Gilbertson and colleagues reported high diagnostic performance for chest ultrasonography in rib fracture detection, with a pooled sensitivity of 89-91% and a specificity of 98-99%. In comparison, chest X-ray misses 50-90% of the rib fractures, depending on fracture location and displacement.
Why This Matters
Accurate diagnosis matters even when rib fracture management is conservative. Confirming a fracture helps clinicians and patients align on expectations, pain control, and precautions. It also supports counseling on warning signs and prevents premature reassurance based solely on a negative X-ray.
POCUS can also expand the assessment beyond the rib itself. In the same encounter, clinicians can evaluate for pneumothorax, pleural effusion, soft tissue hematoma, and muscular injury, without additional radiation.
Impact on the Patient
In this case, ultrasound provided an immediate explanation for the patient’s pain when radiography did not. The diagnosis supported appropriate outpatient management, including anti-inflammatory medications, activity modification, and counseling on the use of an incentive spirometer to reduce the risk of atelectasis. The patient was advised on return precautions, including worsening pain, shortness of breath, or hemoptysis, and was discharged with outpatient follow-up.
Key Takeaway
When focal chest wall pain persists after blunt trauma and the chest X-ray is negative, targeted rib ultrasound over the point of maximal tenderness can identify non-displaced fractures that may otherwise go undetected. This is a high-yield application of POCUS for primary care, urgent care, and emergency medicine clinicians.
For practices considering implementing or expanding POCUS programs, tools such as POCUS ROI Calculators and a POCUS Billing Readiness Checklist can help estimate financial impact and ensure appropriate workflow and documentation processes are in place.
References:
Reference
Gilbertson J, Pageau P, Ritcey B, et al. Test Characteristics of Chest Ultrasonography for Rib Fractures Following Blunt Chest Trauma: A Systematic Review and Meta-analysis. Ann Emerg Med. 2022;79(6):529-539. doi:10.1016/j.annemergmed.2022.02.006
Battle C, Hayward S, Eggert S, Evans PA. Comparison of the use of lung ultrasound and chest radiography in the diagnosis of rib fractures: a systematic review. Emerg Med J. 2019;36(3):185-190. doi:10.1136/emermed-2017-207416
Expert Panel on Thoracic Imaging:, Henry TS, Donnelly EF, et al. ACR Appropriateness Criteria Rib Fractures. J Am Coll Radiol. 2019;16(5S):S227-S234. doi:10.1016/j.jacr.2019.02.019