
What Does the Evidence Show? Lung Ultrasound vs Chest X-ray in Urgent Care and Primary Care
Urgent care and primary care clinicians are increasingly managing patients with respiratory complaints in environments where timely imaging is critical. Pneumonia, CHF exacerbation, pleural effusion, and pneumothorax often require rapid bedside decision-making, yet traditional imaging workflows can introduce delays and operational challenges. At the same time, clinicians face increasing pressure to improve diagnostic accuracy, improve patient experience, and reduce unnecessary antibiotic prescribing for undifferentiated respiratory illness.
Maintaining onsite radiography also carries substantial operational costs for urgent care centers, including staffing, equipment maintenance, regulatory compliance, and quality oversight. In many clinics, ongoing radiography-related expenses can approach six figures annually. While chest X-ray remains an important diagnostic tool, growing radiology technologist shortages and operational constraints are forcing many organizations to rethink how frontline imaging is delivered.
Point-of-care ultrasound (POCUS) is increasingly emerging as a practical solution to these challenges.
Unlike chest X-ray, lung ultrasound provides real-time bedside imaging without radiation exposure or dependence on radiology staffing. More importantly, the evidence consistently demonstrates that lung ultrasound can match or outperform chest radiography for several of the most common cardiopulmonary conditions encountered in outpatient and acute care settings.
Below is what the evidence shows.
Lung Ultrasound Demonstrates Superior Diagnostic Performance Compared to Chest X-ray
Point-of-care ultrasound demonstrates superior sensitivity compared to chest X-ray for pneumonia, pneumothorax, and pulmonary edema, while maintaining comparable or higher specificity across these conditions.
Pneumonia
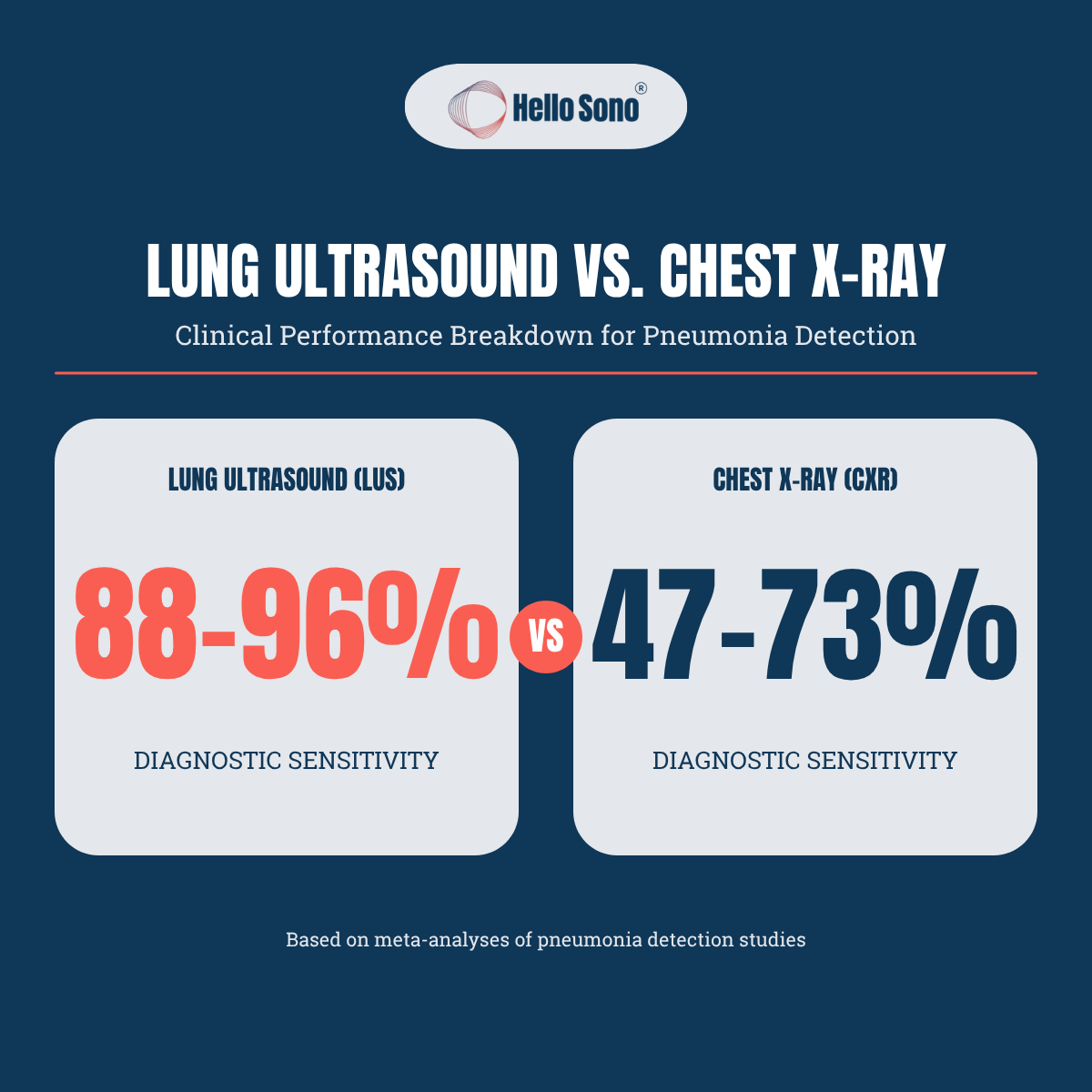
For pneumonia diagnosis, lung ultrasound shows significantly higher sensitivity (88–96%) compared to chest X-ray (47–73%).[1-3]
A 2025 meta-analysis found the BLUE protocol achieved 88% sensitivity for pneumonia detection.[1]
In critically ill ICU patients, a Bayesian network meta-analysis reported lung ultrasound sensitivity of 93% versus chest X-ray sensitivity of 65%, with comparable specificity (83% vs 81%).[4]
Another recent study in emergency department patients with acute dyspnea found POCUS achieved 96.3% sensitivity and 90.4% specificity for pneumonia, with mean time to diagnosis of 16 minutes versus 84 minutes for radiography.[2]
Pneumothorax
Ultrasound demonstrates pooled sensitivity of 75–91% and specificity of 98–99% for pneumothorax, substantially outperforming supine chest X-ray sensitivity of 30–47%.[5-7]
The Society of Critical Care Medicine recommends ultrasound to complement or replace conventional chest radiography for pneumothorax diagnosis (Grade 1A), noting that visualization of comet tails reliably excludes pneumothorax while demonstration of a lung point confirms the diagnosis.[6]
A 2020 Cochrane review of trauma patients found ultrasound sensitivity of 91% versus chest X-ray sensitivity of 47%, with comparable specificities near 100%.[5]
Pulmonary Edema
Lung ultrasound shows superior sensitivity (88–96%) compared to chest X-ray (65–73%) for detecting pulmonary edema.[8-10]
A 2022 meta-analysis found lung ultrasound achieved 91.8% sensitivity and 92.3% specificity versus chest X-ray's 76.5% sensitivity and 87.0% specificity for cardiogenic pulmonary edema.[8]
The American College of Emergency Physicians guidelines note that POCUS assessment for B-lines is 83–92% sensitive and 84–92% specific for pulmonary edema.[11]
How Long Does Lung Ultrasound Take?
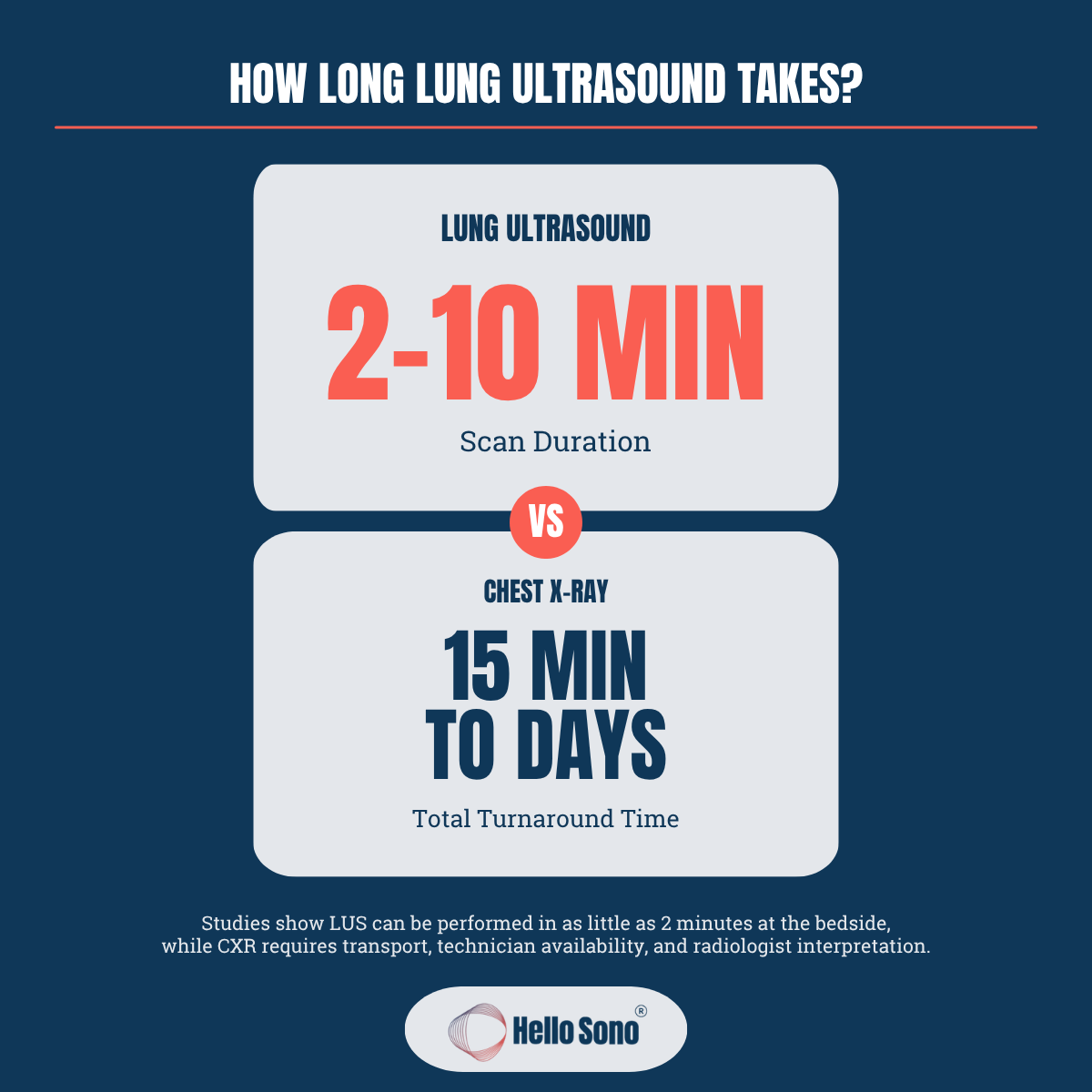
A focused lung POCUS exam for suspected CHF exacerbation can often be performed in approximately 2 minutes using a rapid fixed-zone B-line assessment. In contrast, a more comprehensive pneumonia evaluation typically takes 5–10 minutes, as it involves systematically scanning and characterizing findings across multiple lung fields. [12-13]
Even a detailed lung ultrasound exam is often significantly faster than obtaining a chest X-ray. In a best-case scenario with immediate on-site radiology availability, a chest X-ray may take approximately 15–20 minutes from order placement to image availability. However, in many urgent care and outpatient settings, delays may be substantially longer due to limited staffing, patient backlogs, off-site imaging workflows, or the need to refer patients to an outpatient radiology center.
Why This Matters in Urgent Care and Primary Care
Respiratory complaints are among the most common reasons patients seek care in urgent care and primary care settings.
Yet many clinics continue to rely exclusively on chest radiography, despite growing evidence that lung ultrasound can provide faster and more accurate bedside evaluation for conditions such as pneumonia, pulmonary edema, and pneumothorax.
This has practical implications beyond diagnostic accuracy alone.
Lung ultrasound can help:
Reduce delays in diagnosis and treatment
Improve bedside clinical decision-making
Reduce radiation exposure
Decrease dependency on radiology staffing
Improve patient throughput and operational efficiency
Potentially reduce unnecessary transfers or downstream imaging
Importantly, these benefits are not theoretical.
In a recent utilization and financial modeling study that we co-authored examining adult urgent care visits, approximately 9.2% of encounters were predicted to benefit from POCUS evaluation, with thoracic applications representing a major proportion of potential use cases. The analysis also demonstrated that POCUS implementation can be financially feasible for many urgent care centers when integrated thoughtfully into clinical workflows. [14]
Adoption of lung ultrasound is also becoming increasingly realistic across urgent care and primary care settings. Handheld ultrasound devices have become more portable and affordable, while newer AI-assisted features can help clinicians acquire and interpret images more confidently. Although training, workflow integration, and quality assurance remain essential, these advances are lowering barriers to implementation and accelerating broader adoption of POCUS in frontline care.
As workforce shortages, operational pressures, and demands for higher-value care continue to reshape outpatient medicine, the conversation around POCUS is no longer simply about adopting new technology. It is increasingly about building more resilient, efficient, and clinically capable frontline care environments.
Ready to take the next step with POCUS? Hello Sono helps practices roll out high-quality, compliant, and profitable POCUS programs.
References:
Padrao EMH, Caldeira Antonio B, Gardner TA, et al. Lung ultrasound findings and algorithms to detect pneumonia: a systematic review and diagnostic testing meta-analysis. Critical Care Medicine. 2025. doi:10.1097/CCM.0000000000006818.
Hamza Yousef MS, Al Azizi HM, Fouad MM. Point-of-care ultrasound as a bedside diagnostic tool in acute dyspnea patients in the emergency department for timely management. Respiratory Medicine. 2025;108500. doi:10.1016/j.rmed.2025.108500.
Winkler MH, Touw HR, van de Ven PM, Twisk J, Tuinman PR. Diagnostic accuracy of chest radiograph, and when concomitantly studied lung ultrasound, in critically ill patients with respiratory symptoms: a systematic review and meta-analysis. Critical Care Medicine. 2018;46(7):e707-e714. doi:10.1097/CCM.0000000000003129.
Orso D, Fonda F, Bove T. Lung ultrasound vs chest radiography for pneumonia diagnosis in critically ill patients in the intensive care unit: a systematic review and Bayesian network diagnostic meta-analysis. EClinicalMedicine. 2025;89:103553. doi:10.1016/j.eclinm.2025.103553.
Chan KK, Joo DA, McRae AD, et al. Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department. Cochrane Database of Systematic Reviews. 2020;7:CD013031. doi:10.1002/14651858.CD013031.pub2.
Frankel HL, Kirkpatrick AW, Elbarbary M, et al. Guidelines for the appropriate use of bedside general and cardiac ultrasonography in the evaluation of critically ill patients-part I: general ultrasonography. Critical Care Medicine. 2015;43(11):2479-2502. doi:10.1097/CCM.0000000000001216.
Ron E, Alattar Z, Hoebee S, Kang P, vanSonnenberg E. Current trends in the use of ultrasound over chest X-ray to identify pneumothoraces in ICU, trauma, and ARDS patients. Journal of Intensive Care Medicine. 2022;37(1):5-11. doi:10.1177/0885066620987813.
Chiu L, Jairam MP, Chow R, et al. Meta-analysis of point-of-care lung ultrasonography versus chest radiography in adults with symptoms of acute decompensated heart failure. American Journal of Cardiology. 2022;174:89-95. doi:10.1016/j.amjcard.2022.03.022.
Wooten WM, Shaffer LET, Hamilton LA. Bedside ultrasound versus chest radiography for detection of pulmonary edema: a prospective cohort study. Journal of Ultrasound in Medicine. 2019;38(4):967-973. doi:10.1002/jum.14781.
Maw AM, Hassanin A, Ho PM, et al. Diagnostic accuracy of point-of-care lung ultrasonography and chest radiography in adults with symptoms suggestive of acute decompensated heart failure: a systematic review and meta-analysis. JAMA Network Open. 2019;2(3):e190703. doi:10.1001/jamanetworkopen.2019.0703.
American College of Emergency Physicians. Ultrasound guidelines: emergency, point-of-care, and clinical ultrasound guidelines in medicine. 2023.
Platz E, Lewis EF, Uno H, Peck J, Pivetta E, Merz AA, Hempel D, Wilson C, Frasure SE, Jhund PS, Cheng S, Solomon SD. Detection and prognostic value of pulmonary congestion by lung ultrasound in ambulatory heart failure patients. Eur Heart J. 2016 Apr 14;37(15):1244-51. doi: 10.1093/eurheartj/ehv745. Epub 2016 Jan 26.
Rodríguez-Contreras FJ, Calvo-Cebrián A, Díaz-Lázaro J, Cruz-Arnés M, León-Vázquez F, Del Carmen Lobón-Agúndez M, Palau-Cuevas FJ, Henares-García P, Gavilán-Martínez F, Fernández-Plaza S, Prieto-Zancudo C. Lung Ultrasound Performed by Primary Care Physicians for Clinically Suspected Community-Acquired Pneumonia: A Multicenter Prospective Study. Ann Fam Med. 2022 May-Jun;20(3):227-236. doi: 10.1370/afm.2796.
Weissert J, Russell J, Havryliuk T. Algorithmic prediction of utilization and financial viability modeling for point-of-care ultrasound (POCUS) in adult urgent care patients. Journal of Urgent Care Medicine. 2026;20(5):25-31.